Cortisol Suppression Test (Dexamethasone Suppression) (ACTH suppression)
Cortisol Suppression Test
What sample is needed for the cortisol suppression test?
- Take fasting blood to prepare the serum.
- A 24-hour urine sample is needed.
- Take a baseline 24-hour urine collection for corticosteroids (urine 17-OHCS) or urinary cortisol.
What are the Indications for the cortisol suppression test?
- This test is done to diagnose adrenal hyperfunction (Cushing’s Syndrome).
- This also diagnoses adrenal hypofunction (Addison’s disease).
What are the precautions for the cortisol suppression test?
- Physical and emotional stress can increase ACTH release and interfere with the interpretation of the test result.
- Drugs that will interfere with the results are barbiturates, oral contraceptives, estrogen, Dilantin, steroids, and tetracyclines.
- Explain the procedure to the patients.
- Take the patient’s weight as a baseline for evaluation of the side effects of steroids.
How will you perform the rapid cortisol suppression test?
- This test is easy and quick to perform.
- This is used as a screening test for Cushing’s syndrome.
- Obtain 4 ml of fasting blood at 8 AM.
- Inject I/M or I/V cortisone.
- Collect 5 ml of blood after 30 and 60 minutes of injection.
- Serum or heparinized blood can be used.
- What is the normal value of the rapid cortisol suppression test = Nearly zero cortisol levels.
How will you perform the prolonged suppression test?
- Obtain 24 hours of urine as a baseline sample.
- Collect blood for baseline cortisol level.
- Collect 24-hour urine samples daily for 6 days.
- On day 3, give a low dose of dexamethasone by mouth (with antacid or milk).
- On day 5, give a high dose of dexamethasone by mouth like above.
- Keep the urine refrigerated.
- What is the normal value of a prolonged cortisol suppression test?
- Low dose = >50% reduction of plasma cortisol and 17-hydroxycorticosteroid levels (17-OCHS).
- High dose = 50% reduction of plasma cortisol and 17-OCHS.
What is the protocol for an overnight low-dose dexamethasone suppression test?
- One mg of dexamethasone is given at 11 PM by mouth.
- Collect the blood at 8 AM.
- A normal person’s cortisol concentration is suppressed to 2 µg/dL or less.
- Cushing’s patient does not show suppression, and the level may be >10 µg/dL.
How will you interpret the cortisol suppression test?
- Suppression occurs in patients with:
- Cushing’s syndrome, where the level is >10 µg/dL.
- In 50% of the cases, the cause is endogenous.
- There is no suppression in patients with:
- Adrenal Adenoma.
- Adrenal carcinoma.
- In the case of an ectopic ACTH-producing neoplasm.
- Absent or failure response to cortisol stimulation is seen in:
- Addison’s disease (adrenal insufficiency).
- Hypopituitarism (secondary adrenal insufficiency).
- Adrenal adenoma and carcinoma.
- Responding to cortisol stimulation indicates adrenal hyperplasia (Cushing’s syndrome).

Cortisol Suppression Test: Cortisol secretion and control mechanism
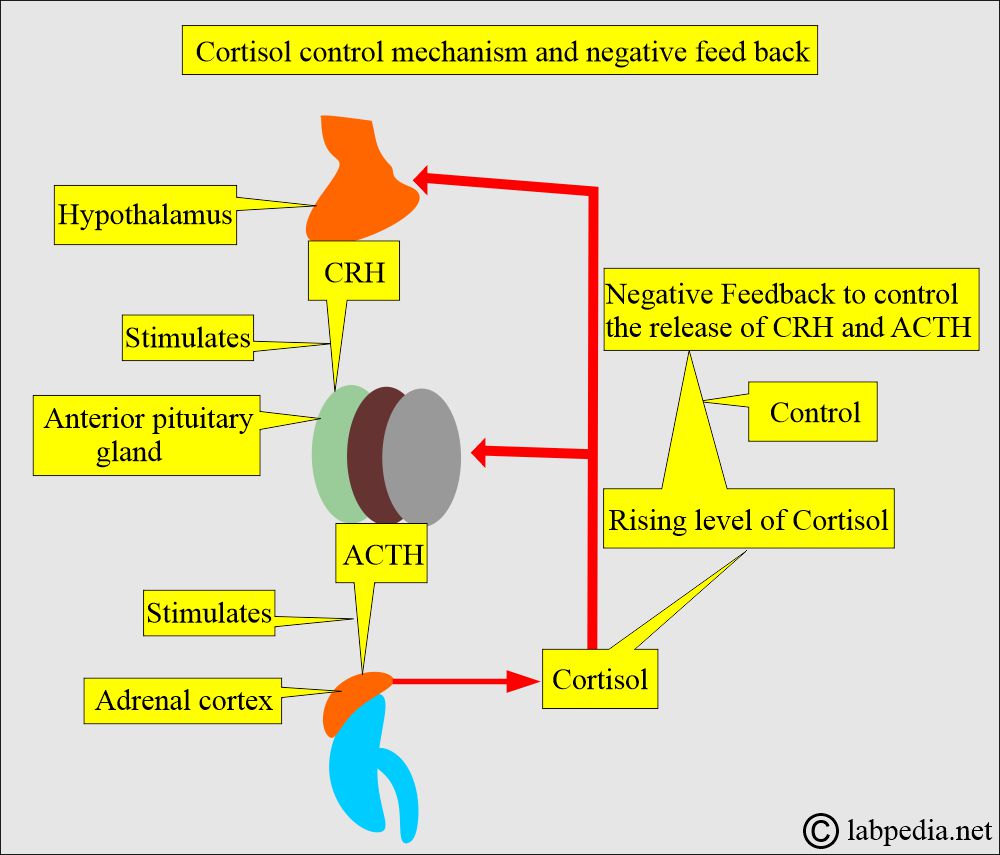
Cortisol control mechanism

Cortisol feedback mechanism
What is the relation of Cushing’s syndrome to the dose of cortisone?
| Disease | Causative reason | low dose | High Dose |
|---|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
What are the causes of Adrenal hyperfunction?
- Cushing’s Syndrome.
- Ectopic ACTH-producing tumors
- Adrenal adenoma or carcinoma.
- Bilateral adrenal hyperplasia.
- Mental depression.
What are the causes of Adrenal Hypofunction?
- Addison’s disease.
- Neoplastic infiltration.
- Granulomatous inflammation, such as TB, histoplasmosis, and sarcoidosis.
- After adrenalectomy.
How will you differentiate adrenal gland tumors?
| Test | Normal | Cushing’s Syndrome | Adrenal tumor | Ectopic ACTH |
|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Supp = suppression.
H.D. = high dose.
Questions and answers:
Question 1: What is the significance of the cortisol suppression test?
Question 2: In what cases is there no suppression of cortisol?